




Thanks to by Drs. Patrick Hickey, Elizabeth Murray and Alastair McAlpine for providing feedback on this article.
Throughout discussions on whether kids should be vaccinated for COVID, one hears comments like: “kids don’t need it” or “they have almost no risk.” Those who say these sorts of things will focus often on the small number of pediatric deaths attributable to COVID as evidence, explaining that even if a child does get very sick they will usually recover.
It’s a poor argument given that vaccination would be one of the best ways to reduce disease burden among children. But if the risk of dying seems small, we should turn to the 80,000 to 130,000 pediatric hospitalizations from COVID. The fact that a child survived doesn’t tell you all that much about their recovery (or lack thereof). Take it from two PICU doctors: “mortality is an imperfect marker…because it is uncommon and uninformative of outcomes in the majority of patients who survive.” It’s common knowledge within their profession that this kind of severe illness can be life-changing (1, 2). They continue:
“We hoped to declare victory and ‘happily ever after’ with improved survival but find there is more to the story. The ugly truth is that since waking up, Sleeping Beauty needs physical therapy, tutoring at school, and her mother has posttraumatic stress disorder. We cannot depend on a clean, dichotomous outcome in pediatric critical illness.”
Our public health efforts have long prioritized keeping kids out of the hospital, even for low-mortality diseases. We introduced or expanded several vaccines in the 2000s that directly targeted and dramatically reduced the main causes of ID hospitalizations (vaccines: rotavirus, pneumococcus, influenza), which were and still are main causes of pediatric hospitalization (respiratory infections and gastroenteritis). But COVID now threatens to reverse our progress. An AAP study found that while typical bronchiolitis, pneumonia, etc. dropped 80%, hospital outcomes (length of stay, ICU use, ventilation rates) were the same. A JAMA study reports a greater toll than for seasonal influenza even before Delta or Omicron.
All of these diseases have the potential for damaging complications. COVID’s complications usually relate to pulmonary dysfunction, but severe COVID shows extensive involvement including cardiovascular and neurological complications. Any severe infection can also trigger a life-threatening immune response called sepsis (AAP review found this in about 5% of hospitalized cases). Infection of the lungs can for obvious reasons beget damage elsewhere.
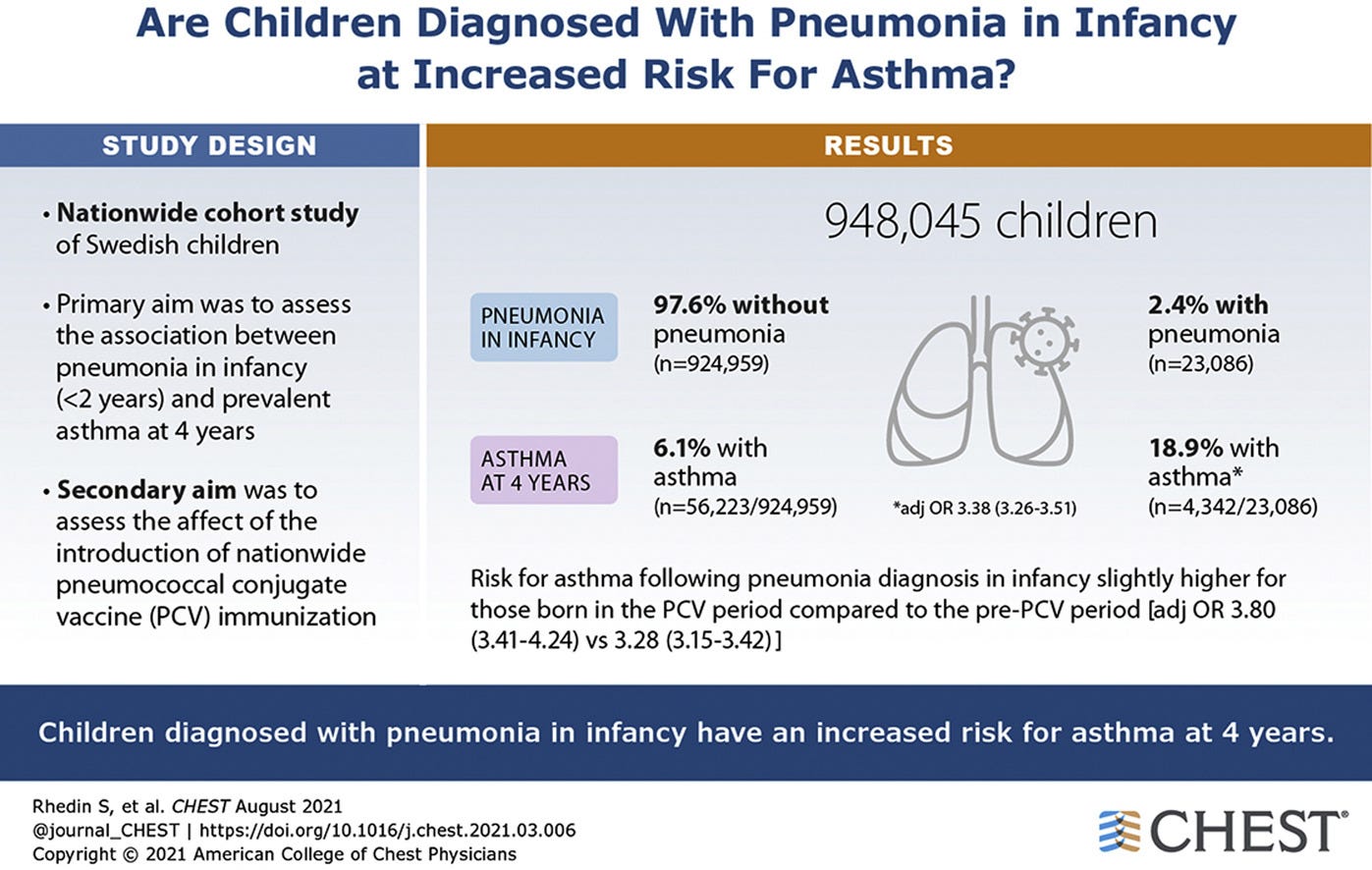
The main pulmonary complications of COVID are pneumonia and acute respiratory distress (ARDS). Pneumonia is the major cause of ARDS, but either might contribute to persistent respiratory dysfunction. Pneumonia in early childhood (<5) is robustly associated both with obstructive lung disease (e.g. asthma) and restrictive lung disease. Some studies even find the correlation to be on-par with smoking. Correlation is NOT causation as kids who get pneumonia are more likely to be at risk for lung disease, but many authors including in Pediatrics, NEJM & Chest argue that is unlikely to explain the whole of the connection. They each make a similar case: “Vaccines against common respiratory pathogens may have longer-term benefits than simply protecting against episodes of acute pneumonia.”
The extent to which this applies to COVID is unclear, which is unsurprising given that research on the long-term effects of acute infection often takes many years to reach consensus. Studies that look at persistent symptoms almost universally follow mild cases. Those in hospitals vary in their findings and rarely follow-up. But from a review of the literature and discussions with pediatric disease experts, COVID pneumonia does not seem much less severe than other viral causes.
For kids who are sent to the ICU with respiratory distress (the most common reason), outcomes are more severe. For example, a study in JAMA found that previously healthy children put on a ventilator showed lower average IQ compared to their siblings. The drop was small albeit still half of what is seen in the case of lead poisoning (whose effect is less about the average and more about standard deviations). This could be due in part to prolonged use of general anesthesia in kids, for which the FDA has issued a tentative warning. But it would be intolerable and traumatic to do this awake so there’s no alternative.
The IQ drop observed came after explicit exclusion of those with devastating neurological consequences. COVID can cause these too. A large review in JAMA looking at 61 hospitals between March and December 2020 found that 22% of kids who were hospitalized had neurological complications, with 12% being severe (2.2% of kids admitted). Most of these kids either had neurological deficits at discharge or died; because they were more likely to survive, those with new disability were mostly healthy going in. Doctors who witnessed these conditions before the pandemic emphasize prevention: “lack of specific treatment for neurologic complications underlines the importance of early diagnosis, use of antivirals, and universal influenza vaccination in children.”
About half of neurological complications stem from MIS-C, which is much less common now (though may reappear in immune-naïve babies). But the remaining half were unrelated. And authors repeatedly emphasize how infection in one place can beget such damage elsewhere. Hence one study found that 5.6% of kids who were ventilated for bronchiolitis suffered cardiac arrest, which is a “known cause of severe neurologic morbidity.”
I could keep going. Doctors report clotting, kidney injury, hepatitis and others. Treatment of severe COVID can involve steroids or broad-spectrum antibiotics (likely with worse side-effects than vaccination). But equally important to what happens in the hospital is what happens after. The injuries that accumulate within often result in a lasting recovery syndrome called post-intensive care syndrome (PICS). Early data suggest that around 23% of kids leaving the ICU are functionally impaired, with half failing to fully recover after 2 years. The most common impairments are serious: difficulty eating, motor dysfunction, cognitive issues, and are thought to primarily stem from actual physical damage to tissue (lungs, brain, muscle wasting, etc.).
We believe that while these problems are rarer in children than adults, they have a greater impact because they occur in a critical developmental window. A child who falls behind as a result of illness may face permanent consequences even if they were perfectly healthy before and go on to make a full physical recovery. Parents may face severe emotional challenges, and caregiving is time-consuming and stressful. We have no research on how this impacts their siblings, broader community, etc.


And more generally, we’re still learning both about how kids recover from the hospital and how their bodies respond to various infections. It is commonly suspected and in some cases known that acute infections play a role in chronic disease (1, 2, 3). A study from Finland found that being hospitalized for an infectious disease in youth is correlated with worse socioeconomic outcomes, with most of the effect coming from missed opportunities. It’s a tenuous connection, but certainly plausible that a child who falls behind may struggle to achieve, have worse mental health (or even trauma), etc. A study for the AAP found that early life hospitalization for disease was correlated with worse metabolic health in adulthood. And as former FDA Commissioner Scott Gottlieb points out:
“COVID is a novel and pathogenic virus. Most kids will have a mild course and recover fine from acute illness. But we should show humility that we don’t know its long term implications. Letting an entire generation of kids get infected, with no baseline immunity, may be imprudent.”
Even if there were no long-term effects from the virus, pediatric hospitalization is likely to be one of the most fearful, stressful and possibly dangerous experiences a child will face. COVID has hospitalized upwards of 100,000 kids in the United States with a ballpark of 20,000 in the ICU. Still some see this and ask: Do kids really need to be vaccinated?
The answer is yes. The US’s Healthy People initiative–our now 42 year framework for continued health improvement–explicitly lists reduction in infectious disease hospitalization as one of its goals. We’ve managed to consistently reduce their burden in kids through the introduction or expansion of several vaccines: pneumococcal vaccines (2000, 2007), expanded flu vaccination (2003, 2006, 2008), and rotavirus vaccines (2006). While most lower respiratory tract infections are not associated with a particular pathogen, we’re on the verge of achieving a vaccine for respiratory syncytial which is the last major identifiable cause without one.
Or… it was.
COVID first circulated while other diseases vanished, but as they return it will join the pathogenic pantheon. I previously argued that not vaccinating for COVID would be out of line with decades-long efforts in public health and vaccinology. This is truer than I knew then. From 1993 to 1994, the CDC put on a major program to vaccinate kids against 14 different diseases, with 6 new vaccines introduced throughout the study period. No single one of these vaccines single-handedly defeated severe disease. Instead each took a significant step forward by targeting a specific pathogen.
Historical reviews suggest this was a proactive step and hard-won deviation from the norm. Where perfect evidence wasn’t available, we still prioritized making kids healthier by using the best evidence at hand. We did this with the HPV vaccine (it’s not ethical to do an RCT where kids get cancer), with some flu vaccines (we use immunobridging rather than clinical efficacy because it’s not ethical to withhold a vaccine we know works in older children), with meningococcal vaccines (certain outcomes are rare so an RCT isn’t always possible), with pneumococcal vaccines (we used Prevnar 7 before Prevnar 13, so a control group didn’t exist), among others.
I see no reason to let ourselves backslide now given that we have a safe and effective vaccine for COVID. In fact, as the population that meets the virus for the first time shifts younger we may see even greater benefit from routine immunization. Rolling this out now will prepare for routine use of improved vaccines in the future. But without intervention, a small number of kids will be disabled or even killed by severe infection, year after year, with permanent consequences for their families.
You need a damn good reason not to intervene. And to date, I’ve mostly seen vague pushback without suggestion of an alternative for how to improve child health. So my advice to you is this: don’t let your child’s health become a liability at the behest of those who are simply trying out arguments. Take the clearest, most effective step available to you to protect them.
Vaccinate.
Related Reading