

Monkeypox: A Full Review


Hello all! This article is reformatted from a Twitter thread I wrote on monkeypox. I know I haven’t posted an article here in a while, but I will have something unique to share in the next week or so. Until then: I hope you still care about monkeypox even if it’s not on the front page (you should)!
The monkeypox outbreak of 2022 has raised lots of questions yet answered few. While now improving, most people feel uncertain about what just happened and where it's all going. A 🧵 on all things MPOX.
I've written this as a timeline, with sections as follows:
1⃣ Outbreak origins
2⃣ US Response
3⃣ STI Comparisons &
4⃣ What's Next? (Endemicity, Evolution, Etc.)
This will be thorough. Feel free to scroll down to one that's more relevant to you.
I wrote this to nail down key points in a time of information overload. I've kept up with coverage to hopefully now distill it down to: how did monkeypox get so out of control and how can we do better?
Chapter 1: A Neglected Pox
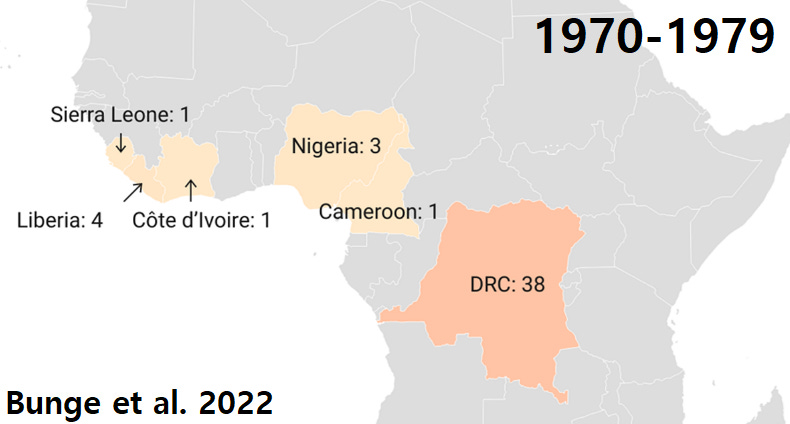
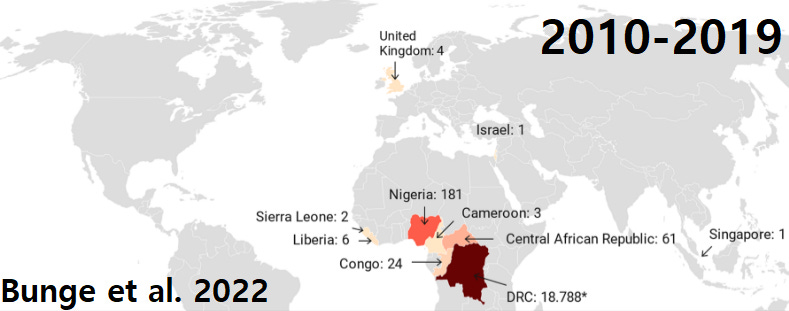
You likely know that MPOX was a virus endemic to certain parts of Africa, to which smallpox vaccination gave immunity. So not long after vaccination programs end in 1980 we begin to see more reported cases.
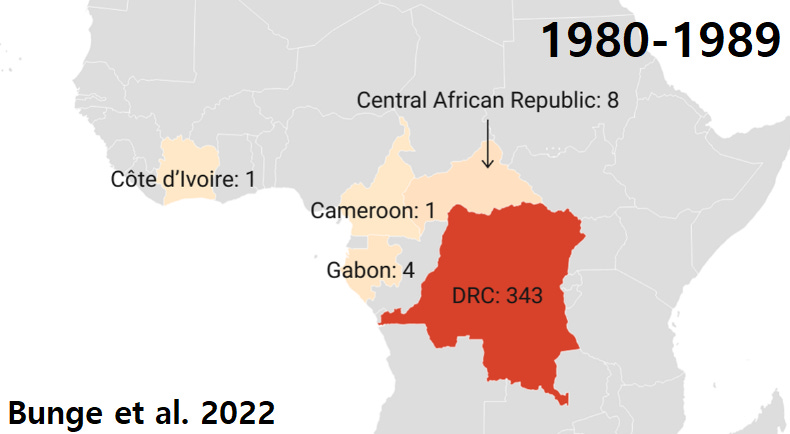
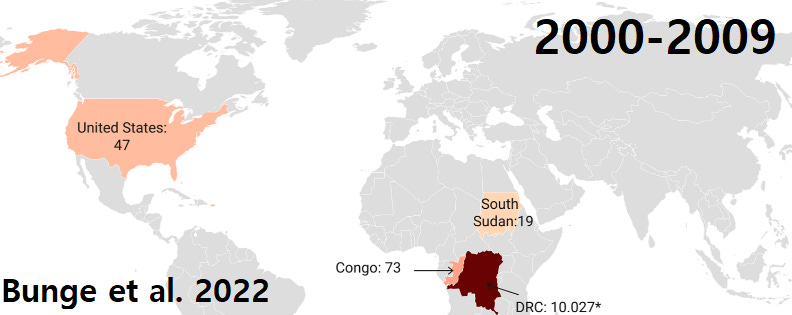
Experts knew in 1988 that this would get worse: "the average magnitude and duration of epidemics will increase.” The 2000s and 2010s affirmed that, though DRC switched to 'suspected' cases.
At the same time, ongoing research pointed to harmful knowledge gaps. A 2003 Nature paper warned we should study its capacity to evolve during outbreaks.
A 2012 CDC paper notes: "fairly minor shifts [could] tip the balance in favor of sustained spread." This is remarkable because they also knew we might not be able to react to such an outbreak.
2017 research which the CDC funded and analyzed samples for concluded that we could not reliably distinguish MPOX from other diseases (specifically including herpes and syphilis).
Fast forward to today. Dr. Jay Varma makes explicit: "The skin changes can also mimic those of herpes or syphilis.” Professor Bill Hanage writes: "folks don't expect to see monkeypox and so don't diagnose it...You see lesions, you assume it is something else.”
Moreover, when Nigeria had an outbreak in 2017 they couldn't determine how MPOX was spreading. Their CDC lead: "In a way, it’s similar to the surprise around the world right now." And yeah, our own CDC concluded in 2018 that we need to strengthen epi capacity there...
Then of course a pandemic happens. But when travel resumes we observe multiple, presumably unrelated MPOX outbreaks in places like the UK. So clearly this pox is epidemic ready.
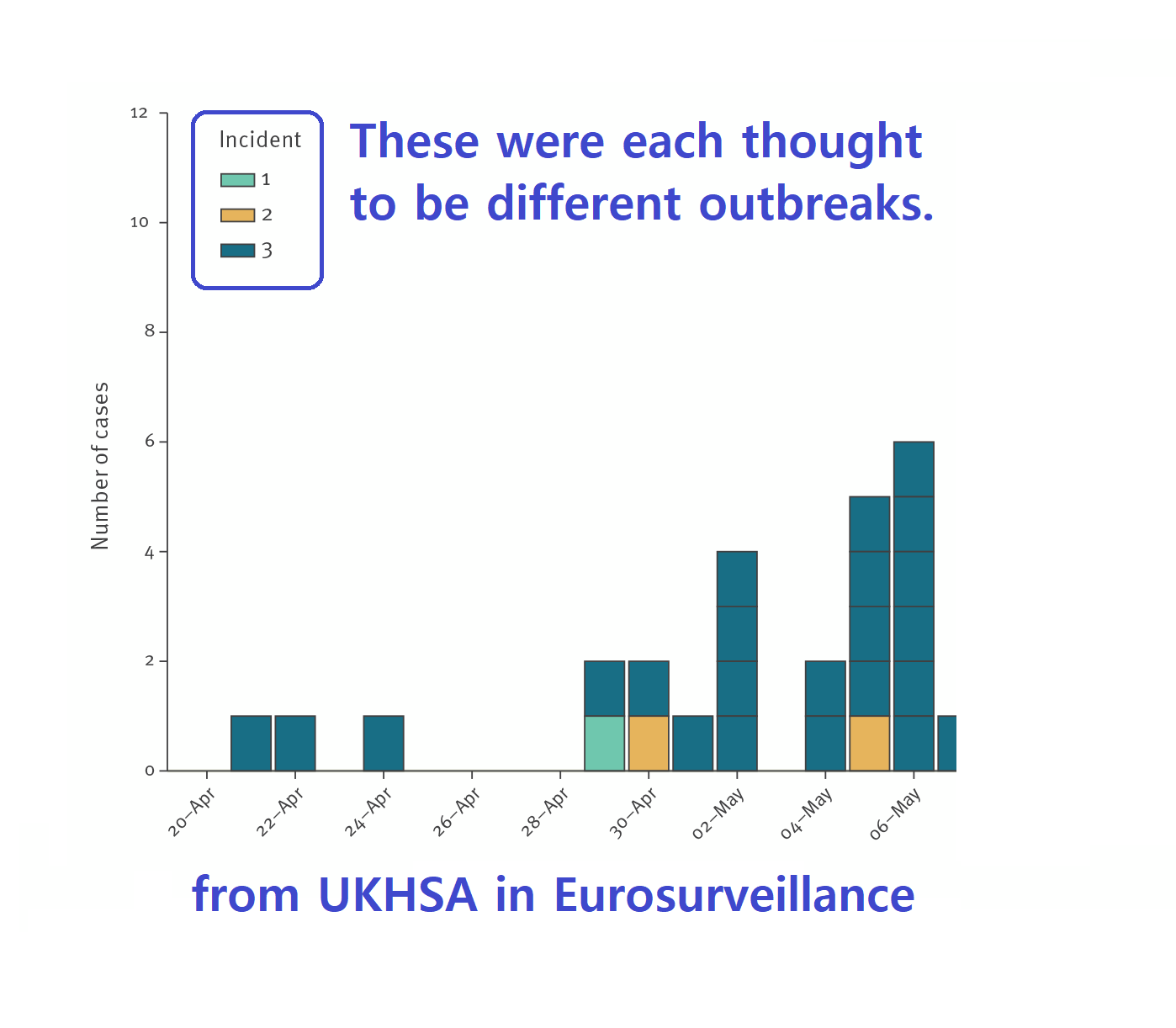
Because in contrast to the "fairly minor shifts" required for an outbreak, societies change fast. Nigeria, e.g., urbanized. You can see how recent cases map onto dense transport hubs.

We also know the world is becoming more interconnected. A 2005 Nature paper showed STI epidemiology sync up between US cities closer to the 21st century as travel increased...
Another study of sexual network 'bridgers' found that in just one US county, people had partners in 13 countries. So a pox that spreads through close contact can still go international these days.

One question remains: did MPOX evolve to become more contagious? Consensus tends toward 'yes,' though clear evidence beyond expert opinion is hard to come by.


Chapter 2: America Fumbles
It's now 2022. The virus CDC worried about is here, and it is sneaky! When the outbreak starts in late May it takes 11 days from when a person gets a rash to when they're diagnosed.
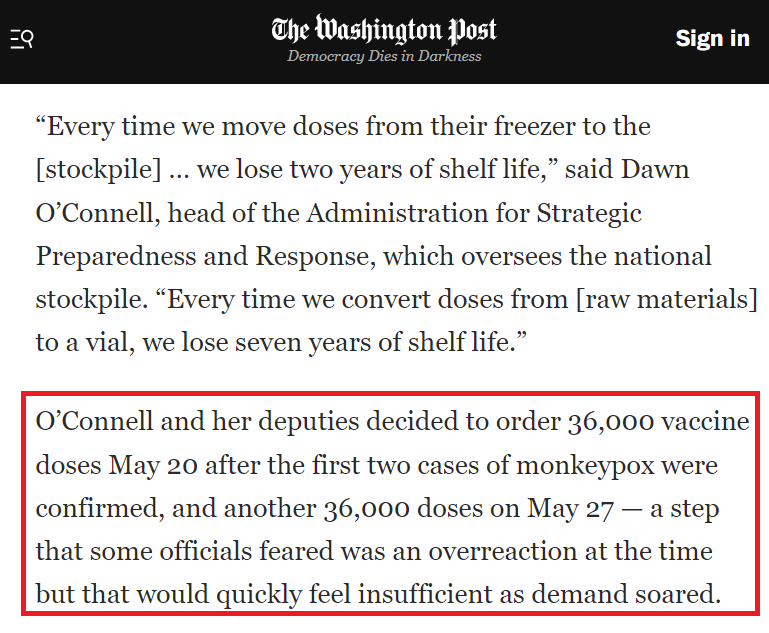
The CDC realizes we're behind, and expands testing by mid-June. HHS follows suit by 'over-ordering' vaccines. Yet their "overreaction" was actually an underreaction to the virus.
So I think they are trying to learn, but too slowly. Institutional habits are sturdy. As virologist Angela Rasmussen notes: "we're just doing the same thing all over again, because that's the way it's done."
On the side of reform, Caitlin Rivers has detailed how CDC has been more open with their data. She herself has proposed testing strategies to address blind spots. And she's bringing that skill as associate director for CDC's new forecasting center.

And we can't only focus on health agencies. In the US, sexual health clinics are underfunded even as STIs go up. Jay Varma noted in June that an estimated 1 in 5 Americans has one.
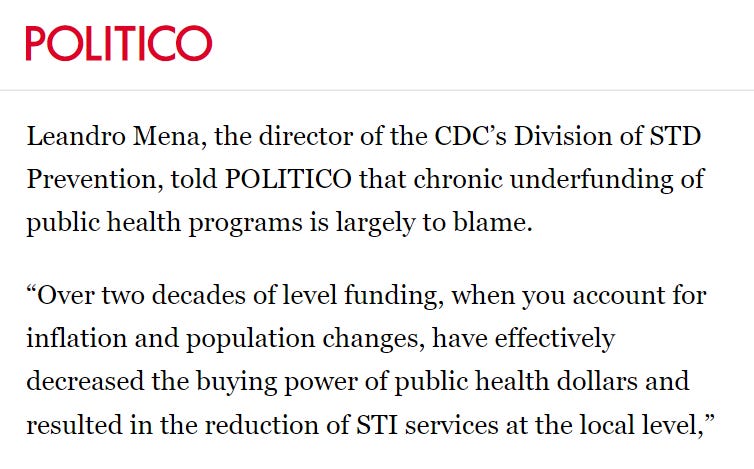
Meanwhile, CDC's STI prevention branch has actually lost spending power *for two decades.* Thus ID docs at STI clinics we’re saying things like: "monkeypox testing & PEP are increasing exponentially. Not in our budget, and we don't have the staff.”
In case lawmakers claim they've given enough $$, I quote the clinical lead at the Detroit STD clinic: "Everyone's doing overtime without getting paid for it, because no else can do it."
This also shows up in treatment. Doctors from IDSA have noted it takes hours of paperwork to get TPOXX for a patient, a task left to already rare ID physicians (alongside COVID)!
That's no small deprivation for patients. IDSA's @DrMaryFoote said: "the morbidity has been higher than any of us expected."
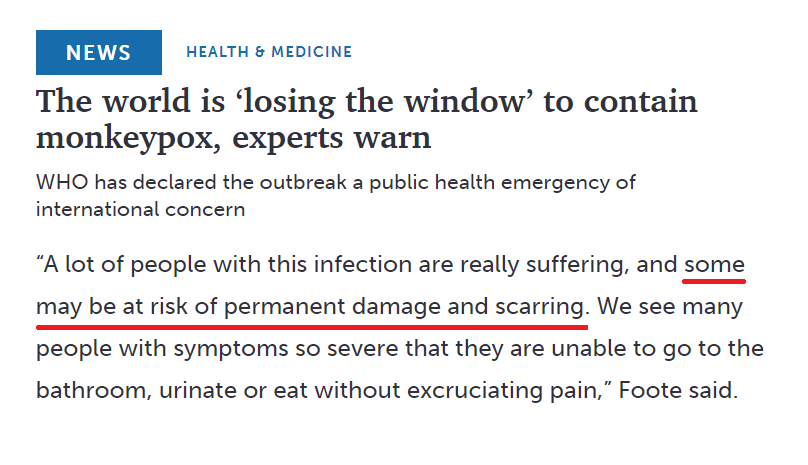
Foote later followed up-with NBC, noting some cases may need surgery (in part because MPOX can scar the eyes & genitals). Yet because it’s a neglected disease & blends with common STIs, patients have had trouble getting care.
And longstanding STI neglect creates bigger issues. The historical trend (shown below) is that new technologies or interventions bring cases down but then stall at a new baseline. (26)

At that point we have to reach deeper into more diverse communities, so difficulty increases as the perceived problem shrinks. Gregg Gonsalves calls it our vanishing "appetite" to help.
That's a political problem which has long been severe for STIs, but during COVID national solidarity against disease in general took a dive. Vanishing shared will leads to overdependence on technical solutions.
Which not only applies to COVID, but monkeypox too. Yes we have a 💉 but we don't know: how well 1) one dose and 2) intradermal doses work for 3) high-dose exposure (sex).
In fact, a recent study gives reason to wonder how long the two dose series protects. Which leaves us in what Natalie Dean calls an 'evidence limbo.’ And that's a problem because CDC scientists acknowledge STI interventions have a similar issue.
Both uncertainties could have been reduced literally just by addressing the problem earlier. Ranu Dhillon says of MPOX: "The original sin of this whole pandemic is that we could have tested these things in endemic countries, and then we would have the data.”
But because we're re-testing our apparatus to address STIs, we might use past events to peer into the future. (PS: Please get vaccinated if eligible! Uncertainties concern transmission, but it's clear it will help protect your health).
Chapter 3: STIs & Public Health Flaws
For the sake of strategy MPOX is like an STI:
Vax eligibility roughly matches that for PrEP (HIV prevention).
Efficacy studies have been paired with ongoing STI research.
CDC models transmission with models for other STIs.
It also disproportionately impacts men with HIV. This matters as a key fact about STIs is their extremely disparate impact. 42% of new HIV diagnoses are among black men.
Likewise, a CDC paper ranking the greatest health disparities impacting African Americans found 6 of 10 are STIs. Which—and this is going somewhere—is NOT related to behavior:
"Public health efforts have been guided by the premise that the best way to prevent STDs is by targeting risk behaviors. However, the current finding derived from a large, nationally representative sample indicates this strategy may be appropriate for Whites (because their STD risk increases only when their behavior is very risky) but not for blacks. Our results suggest that Black young adults are at very high risk for STDs, even when their behavior is normative.”
That's because it has to do with networks, not individuals. In the case of HIV: we used our technical solution (medication) on white populations which created a then self-reinforcing disparity.
This mechanism of entrenchment and all it entails is still alive. Thus monkeypox has: "spread like wildfire through sexual networks, as HIV did — and continues to do.”
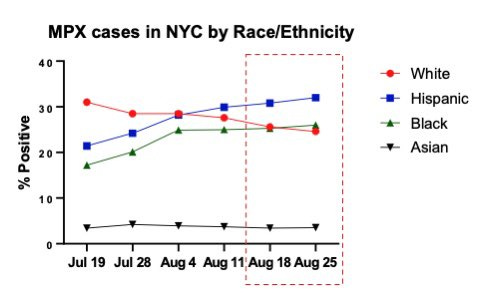
We do see behavior change happening, which can make a large short-term difference (most of the current decline). But we're also seeing case disparities by race.
And because vaccine inequities are already remarkable, the question is what happens when behavior change inevitably reverses.


The MPOX team is of course aware of this long standing problem. Dr. Demetre addressed it last month, now new overall cases are down 85% since the peak. He credits: "community engagement, science and political will.”

Ofc, communities aren't monolithic. I noted Detroit STI clinics are in trouble, with big disparities by race. It's deja vu because Flint (nearby) has a dream-team COVID equity group. Yet vax disparities persist, w/ demographic data hard to even find.
I don't know that we have national data on MPOX case disparities, because when you check the CDC site there's uh... nothing. So I remain somewhat uncertain about how successful outreach is or will be.
This isn't the fault of people like Dr. Demetre. His remarkable work—and that of many in the LGBT community—is a way to make up for some of our longstanding problems. However: individual competence usually isn't enough to solve systemic issues.

Flint, for example, hasn't had many MPOX cases. But from my interactions with the health dept, they're still using the opportunity to improve outreach to black LGBT people. That's the right idea: we should strengthen equity on STIs whether or not this one overwhelmed us.
Because I don't actually think that current inequities will be enough to cement MPOX in the US. But that if it is eliminated, it will be in spite of our record on STIs. And some of that has to do with the virus itself, whose properties will also govern what happens next.
Chapter 4: Monkeypox Futures (and More…)
Monkeypox—we've come to learn—is not good at being an STI. Quoting Jay Varma once again: "None of us who work in public health thought the sky was going to be falling from monkeypox...just concerned that a lot of people were going to suffer."
CDC said at the beginning of September that the outbreak would fizzle in a few months, but "low-level transmission could continue indefinitely.” Dr. Caitlin Rivers adds that elimination in non-endemic settings w/out vaccines could take years.

The mechanism for rebound has been well-illustrated by Ranu Dhillon, who shows that without fully suppressing a disease you leave room for hotspots in harder-to-reach communities.

That's unlikely here, but the virus could evolve anywhere. How big a threat is that? While DNA viruses like MPOX have a mutation rate well below RNA viruses, that's not all that matters.
A 2015 paper in Cell tried to explain how DNA viruses quickly adapt to new species. They discovered that poxviruses gain and lose genes with ease to modify traits.
This is a normal process for the virus, though could perhaps lead to a more serious variant. Some researchers argue that gene loss might help MPOX specialize to humans.
They use smallpox as an example. Most modern pox viruses are thought to have diverged from a common ancestor: cowpox. The theory is smallpox became the dominant one in humans because it trimmed its genome.
The 2012 CDC paper cited earlier makes clear that while smallpox is "not a trimmed-down version of monkeypox," it could show a degree of 'convergent evolution' (reaching similar traits thru different pathways).
That might make it more harmful / transmissible, but how much (and under what conditions) is unclear. The WHO's Mike Ryan thinks endemic transmission in new species is the big risk.
Virologist Stefan Rothenburg makes the same case: "An expanded virus reservoir greatly increases the risk that more adaptive mutations will arise, for example after recombination with other poxviruses."
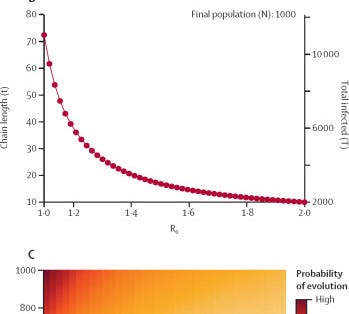
Another argument says that long chains of monkeypox give it a long runway to adapt. A disease like COVID branches off quickly whereas individual MPOX cases chain together better.

I personally would argue the greatest risk is a big shift, with endemic spillover/spillback as one explanation. Another is global transmission in settings without good healthcare.
For example, Omicron may have resulted from a chronic COVID infection in a person with uncontrolled HIV. But even if it didn't, the other popular explanation was evolution after zoonotic spillback!

And the next after that was transmission in a geographically isolated population, which monkeypox already affects plenty of. All of these risks—like with COVID—represent global health vulnerabilities.
"Any containment will be temporary if the rest of the world keeps struggling," says Tom Inglesby. “The future of monkeypox in America is unavoidably linked to the future of monkeypox in the rest of the world.”
We know MPOX would be hard if not impossible to contain if it got into animals. Microbiologist Jason Kindrachuck draws analogy to Ebola: "We’ve been looking for infections for decades now. You're looking for a tiny, tiny pin in a massive haystack.”
So our best bet is to *stop* the outbreak in newer settings and help strengthen surveillance in endemic settings. On the vaccine front we failed, in part because the IP holder won't let African vaccine manufacturers make more...
And also because the US let the majority of Jynneos doses ever manufactured expire over the years instead of using them to help where the disease was endemic (we're not alone: Japan has its own stockpile of vaccines it has declined to share).
We actually seem to have failed from the start in that the US funded Jynneos but left Bavarian Nordic with all the power over its creation and use. E.g. they threatened to stop supplying to us because we were stretching supply via intradermal administration.

But whether or not we can work something out with them, we also have to strengthen regional epidemiological capacity. One of the best examples of what this looks like comes from South African scientist Tulio de Oliveira.
He and colleagues lead research on infectious disease outbreaks through CERI, but in an intensely applied manner. During COVID (before CERI) they: "trained over 5000 medical doctors and nurses between March and August, 2020" on how to avoid hospital outbreaks.
"We probably spend half of our time and 20–30% of our budgets to give feedback to clinicians and do training," he notes. It reminds me of my colleagues at TEPHINET, a CDC/WHO-funded initiative whose work is to train epidemiologists around the world.
We ought to intensify these kinds of programs, and in fact we are. Public-private partnerships are emerging to meet unfilled needs. But most importantly for the reader: we need federal funding.
Because exactly like neglect of STIs in the US today, our government makes intentional policy choices to limit funding. For instance: most of our Ebola response funding went to containment/research. That's likely part of why we're better able to handle outbreaks today.
But that amount came from a consistently limited pool of disaster response funding, negotiated ad-hoc by Congress. And at that point it's obviously too late. So in closing I have two recommendations.
For ordinary people: pay attention to if your representatives are proactive on issues of public health. If not, make clear you care about that.
For scientists: point out to your audience where gaps exist and how they can—specifically and actionably—support policy change.
Because ultimately, the vulnerabilities monkeypox exposed haven't changed despite the outbreak's decline.
Whether it goes away, evolves, another virus pops up, or whatever, something will eventually be too much for fractured health systems to handle.
Now is the time to convert a response into infrastructure, as so many global health experts have told me. We really shouldn't need a virus to bring us to our knees to do that.
The claims in this article are mine alone. If you found it useful, please consider sharing as it takes a lot of time to put these projects together.